- Elbow Anatomy
- Elbow Pain Causes
- Elbow Pain Treatments
- Stretching & Exercises
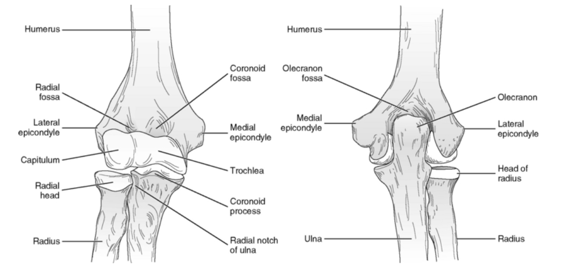
The elbow is a hinge joint. The arm bone (humerus) is connected to the forearm bones (radius and ulna) by various muscles, ligaments (connecting bone to bone) and tendons (connecting muscle to bone).
The Olecranon is the bony prominence on the back of the elbow which is a projection of the ulna bone. Many ligaments help stabilize the elbow. The ulnar collateral ligament (UCL) lies on the inner aspect of the joint with the palm facing forward (ulnar aspect). The lateral collateral ligament (LCL) lies on the outer aspect of the joint with palm facing forward (radial aspect). The UCL protects the elbow against excessive inward (valgus) force and the LCL protects the elbow against excessive outward (Varus) force.
The inner surfaces of the elbow joint are lined with cartilage which is a tissue with a smooth, rubbery surface meant to provide shock absorption and minimize friction during motion. The elbow joint also contains synovial fluid which acts as a lubricant within the joint.
Many muscles attach around the elbow joint. The extensor muscles of the wrist and hand insert at the lateral epicondyle of the humerus. The flexor muscles of the wrist and hand insert at the medial epicondyle of the humerus. The biceps muscle inserts onto the radius below the elbow joint and the triceps muscle inserts onto the olecranon of the posterior ulna.
Lateral Epicondylopathy
Lateral epicondylopathy or “tennis elbow” is the most common diagnosis in patients with elbow pain. Many muscles that work to extend the wrist and fingers form a common tendon which inserts at the lateral epicondyle. Repetitive and long term loading can lead to degeneration and pain in this tendon. It is common in racquet sport players, particularly when a one-handed backhand is employed. However it can also be seen in other athletes and manual laborers.
Pain on the lateral side of the elbow and weakness to the extensor muscles of the forearm are the most common symptoms. The onset of pain can be gradual or sudden and can affect common daily activities such as turning a doorknob, shaking hands or holding a cup.
Medial Epicondylopathy
Medial epicondylopathy or “golfer’s elbow” occurs following repetitive and long term loading to the wrist and finger flexor muscles. This causes tendon degeneration and pain where the flexor tendons insert at the medial epicondyle of the elbow. It has traditionally been associated with golfer’s who take a large divot on their swing or climbers who place large loads on their tendons due to grip. However, like tennis elbow, golfer’s elbow can also occur in any athlete or manual worker.
Pain to the inside of the elbow with the palm up and weakness to the flexor and grip muscles of the forearm are common. There are multiple important structures in close proximity to the common flexor tendon on the inside of the elbow and your physician will check the ulnar elbow ligaments for insufficiency and evaluate the ulnar nerve.
Triceps Tendinopathy
Triceps tendinopathy is a relatively uncommon cause of posterior elbow pain. It occurs secondary to repetitive and long term loading of the triceps tendon. It can be seen more commonly in throwers, weight lifters and gymnasts. Pain occurs on extension of the elbow (straightening the arm). The pain can be felt in the triceps tendon or over the bone itself of the olecranon where the tendon inserts.The Achilles tendon is located at the back of the foot and connects the calf muscles to the heel. Contraction of the calf muscles pulls on the Achilles tendon and allows you to go on your tip-toes (plantar flexion). Pain in the Achilles tendon is a common complaint and is often caused by Achilles tendinopathy. There are two main types of Achilles tendinopathy: insertional (where the tendon meets the bone) and non-insertional (at the middle of the tendon). Non-insertional is the most common type.
Elbow Pain Treatments
Treatment for tendinopathy is similar regardless of the location of the tendon in the body.
- Following an acute injury or flare of pain: rest the affected elbow by avoiding any
offending activities. - Ice may be applied for 15 minutes, 3-4x per day to decrease swelling and pain.
- Acetaminophen and NSAID anti-inflammatories can also be used for pain management.
- Stretching and exercises with a focus on eccentric exercises are the foundation of treatment. They can heal and strengthen the tendon decreasing the risk of recurrent injury in the future.
- Multiple adjuncts are available in the treatment of tendinopathy:
- An elbow strap brace can reduce pain in medial and lateral epicondylopathy by decreasing load placed on the tendon during everyday activities and non-focused exercise/therapy.
- Extracorporeal shockwave therapy (ESWT) has a growing body of evidence supporting it’s use as a treatment for tendinopathy. An ultrasound is used to create micro-damage which stimulates blood flow to the affected area.
- Topical glyceryl trinitrate (Nitro patch) is a patch placed on the skin over the insertion point of the affected tendon. It stimulates blood flow to the area and has been shown to decrease pain in some patient with tendinopathy.
- Cortisone injections can reduce pain with the goal of allowing the affected individual to perform the recommended exercise program. However corticosteroids weaken tissues and can lead to further tear and the potential for tendon rupture. They have also been shown to have a neutral or even negative effect on long term pain scores in lateral epicondylopathy.
- Hyaluronic acid (HA) injection is relatively recent treatment option available for tendinopathy. Evidence is limited however it has been shown to be a safe therapeutic option which may improve pain and recovery.
- Platelet rich plasma (PRP) injection involves separating plasma and platelets from the red blood cells in a blood collection. This injectate, which contains a number of growth and healing factors, is then injected into the affected area of the same patient. It likewise has limited evidence but may improve pain and recovery in tendinopathy.
Elbow Stretches:
Stretches:
Stretching exercises are recommended for the elbow and wrist joint. They help improve the
range of motion of the joint and prevent stiffness. These stretches can be included as part of a
warm up before targeted exercises or activities involving grip such as gardening, golf or tennis.
Follow the video to view how to perform this exercise. Perform a minimum 15 second stretch
of each for 3 cycles.
Wrist Extension Stretch – straighten the arm and extend the elbow completely. Then bend the
wrist upwards as if signaling someone to stop. Use the opposite hand to pull your fingers
towards you until you feel a stretch and hold for 15 seconds.
Wrist Flexion Stretch – straighten the arm and extend the elbow completely. Then bend the
wrist downwards so the fingers are pointed at the ground. Use the opposite hand to pull your
fingers towards you until you feel a stretch and hold for 15 seconds.
Exercises:
Strengthening exercises, with a focus on eccentric (muscle activation with lengthening) help
improve muscle and tendon strength and prevent future injury.
Each exercise should be done 10 times for 3 cycles.
Wrist extension drops: Start with the elbow bent 90 degrees and the forearm supported on a
table with your wrist placed at the edge. With the wrist fully extended slowly lower a dumbbell
(starting at 1 to 3 lb) over 3 seconds. Use the opposite hand to help push the wrist up as far as
possible. Then, without assistance, slowly lower the weight until the wrist is flexed again. As
this movement becomes easier increase the weight and do the exercise with the arm fully
straightened and no longer supported by the table.
Wrist flexion drops: Start with the elbow bent 90 degrees and the forearm supported on a table
with your wrist placed at the edge. With the wrist fully flexed slowly lower a dumbbell (starting
at 1 to 3 lb) over 3 seconds. Use the opposite hand to help push the wrist up as far as possible.
Then, without assistance, slowly lower the weight until the wrist is extended again. As this
movement becomes easier increase the weight and do the exercise with the arm fully
straightened and no longer supported by the table.
Wrist supination strengthening: Start with the elbow bent 90 degrees and the forearm
supported on a table with your wrist placed at the edge. Begin with the palm facing to the side.
Hold either a dumbbell or a kitchen pan. Slowly turn the wrist over 3 seconds so that the palm
is facing down. Then use the opposite hand to help push the weight back to the starting
position. As this movement becomes easier increase the weight and do the exercise with the
arm fully straightened and no longer supported by the table.
Stress ball squeezes – 3 cycles of 10 repetitions
Finger stretch: wrap an elastic band around your 4 fingers excluding the thumb. Splay open and
closed the fingers for 3 cycles of 10 repetitions.
Eccentric elbow extension: Start standing with your arm straight, raised above your head with a
dumbbell or other weight in hand. You can support your arm by placing your opposite hand on
your upper arm below the elbow. Slowly bend your elbow and bring the weight behind your
head. Assistance can be used to straighten your arm again and repeat. Increase weight as the
exercise becomes easier.